Creative Commons Reconocimiento-NoComercial 4.0 Internacional

GAPP, número 27, noviembre de 2021
Sección: EXPERIENCIAS Y CASOS
Recibido: 26-01-2021
Modificado: 02-08-2021
Aceptado: 28-09-2021
Publicado: 12-07-2021
DOI: https://doi.org/10.24965/gapp.i27.10902
Páginas: 101-114
Coordination and crisis management1. The case of the federal Government and two sub-national governments in Mexico2
Coordinación y gestión de crisis. El caso del gobierno federal y dos gobiernos subnacionales en México
Jorge E. Culebro Moreno
Universidad Autónoma Metropolitana (México)
ORCID: https://orcid.org/0000-0002-1200-4469
jcmoreno@cua.uam.mx
NOTA BIOGRÁFICA
Profesor del Departamento de Estudios Institucionales de la UAM-Cuajimalpa, Coordinador del Cuerpo Académico Gestión Pública y Desarrollo Social, y del programa de investigación sobre gestion de crisis. Doctor Polit Universidad de Bergen, Noruega, SNI Nivel II, Research Fellow del Centro para Investigación y Diseño Organizacional de la Universidad Estatal de Arizona. Regulación, reforma administrativa, análisis institucional y organizacional, Coordinación y Gestión de Crisis y Desastres.
Benjamín Méndez Bahena
Instituto Politécnico Nacional (México)
ORCID: https://orcid.org/0000-0001-7046-4992
bmendezb@hotmail.com
NOTA BIOGRÁFICA
Profesor-investigador del Centro de Investigaciones Económicas, Administrativas y Sociales (CIECAS) del Instituto Politécnico Nacional, colabora en el Doctorado en Innovación en Ambientes Locales (DIAL) y la Maestría en Economía y Gestión Municipal (MEGM). Línea de investigación, gestión pública, coordinación institucional entre los organismos de vivienda o de salud, innovaciones sociales, Miembro del Sistema Nacional de Investigadores, nivel 1.
Pablo Cruz
Universidad Autónoma Metropolitana (México)
ORCID: https://orcid.org/0000-0002-8455-0418
stolzcross@hotmail.com
NOTA BIOGRÁFICA
Doctorante en Ciencias Sociales y Humanidades, Universidad Autónoma Metropolitana-Cuajimalpa, Enfoque de estudios en el área organizacional/institucional (UAM). Maestro en Economía y Gestión Municipal (CIECAS-IPN). Estancias de investigación en las universidades de Oslo (2017) y Leiden (2019). Áreas de investigación: análisis institucional, organizacional, instituciones informales, gestión de crisis.
ABSTRACT
The article analyzes how the Mexican subnational3 governments responded the COVID-19 outbreak during the first stage of the crisis. The response of two subnational governments whose territory is part of the largest metropolitan area in the country that has been the focus of the pandemic is presented. We ask about the coordination instruments to face COVID-19 between the federal policy and programs with the subnational governments and argue that, during the first stage of the management of the COVID-19 crisis the institutional and organizational design of the Mexican political-administrative system has had a relevant impact on the government’s response, as well in the coordination policies. The article demonstrates that in a crisis, coordination instruments do not depend on political parties but consist of a blend of weak and suitable articulation of policies of the subnational governments with the federal strategy, as well as the need to improve the instruments of collaboration between the various levels of government in the context of a healthcare system in transformation.
KEYWORDS
Coordination; Governance; COVID-19; Crisis Management.
RESUMEN
El artículo analiza cómo respondieron los gobiernos subnacionales mexicanos al brote de COVID-19 durante la primera etapa de la crisis. Se presenta la respuesta de dos gobiernos subnacionales cuyo territorio forma parte de la mayor área metropolitana del país que ha sido foco de la pandemia. Nos preguntamos acerca de los instrumentos de coordinación para enfrentar el COVID-19 entre la política y los programas federales con los gobiernos subnacionales y argumentamos que, durante la primera etapa de la gestión de la crisis del COVID-19 el diseño institucional y organizacional del sistema político-administrativo mexicano ha tenido un impacto relevante en la respuesta del gobierno, así como en las políticas de coordinación. El artículo demuestra que, en una crisis, los instrumentos de coordinación no dependen de los partidos políticos, sino que consisten en una combinación de articulación débil y adecuada de las políticas de los gobiernos subnacionales con la estrategia federal, así como de la necesidad de mejorar los instrumentos de colaboración entre los gobiernos subnacionales en el contexto de un sistema de salud en transformación.
PALABRAS CLAVE
Coordinación; Gobernanza; COVID-19; Gestión de Crisis.
SUMARIO
INTRODUCTION. I. CRISIS AND COORDINATION. II. COVID-19 CRISIS MANAGEMENT. THE FEDERAL STRATATEGY. III. THE RESPONSE OF THE SUBNATIONAL GOVERNMENT. CONCLUSIONS. REFERENCES.
INTRODUCTION
The first case of COVID-19 in Mexico was diagnosed on February 28, 2020, and two weeks later the federal government began its most important strategy against the COVID-19 outbreak on March 13. This strategy was known as the “National Campaign for Healthy Distance”, and consisted in a social isolation policy, from March 23 to May 30, when the country was still in the second phase of the pandemic (i.e. local transmission). The strategy included three central measures: suspension of activities in the education system, temporary closure of companies defined as non-essential, and interruption of recreational activities, and additional prevention measures related to hygiene and protection were put in place to support vulnerable populations. Almost simultaneously, state governments established further actions, including limiting access to shopping centers and public markets, authorizing home-delivery services for restaurants, and limiting or closing access to cemeteries. This strategy took place in the context of a process of transformation of the public sector in Mexico, in which policies have been directed towards austerity in the public sector. In the case of the health sector through the disappearance of the so-called social protection system in health, known as “Seguro Popular” converted in the Institute of Health for the Well-being (INSABI).
In a country of more 230,000 deaths one year after the pandemic according with the official information, the analysis of the first responses is crucial. The case of México is interesting and has important contributions to the analysis of crisis management as well as policies related to the COVID-19 outbreak. Firstly, because there are few studies have focused on the role of local and subnational governments versus national strategies; and secondly, due to the paradoxical way the coordination instruments in a fragmented system (Bode and Culebro, 2018), the Mexican government confronts the challenge of reducing the impacts of the crisis in a framework of multilevel governance.
Methodologically, the article follows the strategy of qualitative case studies (Ragin, 1999; Stake 1995). Cases which were selected for their ability to explain the importance of coordination instruments, as well as for the complexity and representativeness they have for the Mexican Republic, since they share metropolitan areas, industrial corridors, a large population, and the differentiation of political leaderships (Yin, 1994). Mexico City and the State of México were chosen for several theoretical and empirical reasons. First, because these two cases have been the center of the pandemic governed by different political parties that challenges the idea of political affinity to achieve coordination, as well as the interorganizational capacity of the public agencies (Pavlovic et al, 2021). The design and urban planning of large metropolis have had a relevant impact on the development of the pandemic on different phases of crisis management (Lai et al, 2020; Ribeiro et al, 2020). Second, the existence of a centralist path dependence in Mexico that contributes towards a high specialty hospital infrastructure (Culebro, Méndez and Cruz, 2019). As is noted by the historical institutionalism, further policies would be determined by previous decisions (Moloney and Moloney, 2020). Third, the relevance of the theoretical implications to study a metropolitan area in front of a crisis scenario to reduce the impact of the crisis. in a fragmented health system. The complexity and representativeness that both entities have in the Mexican Republic, by sharing metropolitan areas, industrial corridors, a large population, and the differentiation of political leaderships gives them a unique interest to study coordination in the face of the challenge situation.
The information was obtained mainly from public documents of the three levels of government, and from government sources and databases, among others from Internet portals specialized in COVID-19 of each State, and the daily press conferences. The analysis of legislation was relevant for the study of the intuitional design of both national and state health systems. We conducted what is called a desk research interested in the background and development of historical events (Van Thiel, 2014).
The crisis response to the pandemic has challenged both the governmental capacities, such as the structures and resources available to deal with the critical event; as well as legitimacy, or the perception and media citizen evaluation of how the government copes with crisis (Christensen and Laegreid, 2020). Due to the social pressure towards political actors, there has been a great desire to take impulsive, fast, large, and spectacular measures (Boin and Lodge, 2021a), which may not bring the expected benefits. However, due to the long term of the COVID-19 crisis, we can differentiate two key moments in its management.
The first phase faced a scenario of uncertainty about the scope and impact of the crisis, some governments were not prepared or under underestimated the dangerousness of the virus which was compared, for different reasons, with a small flu (cf. Rucker and Costa, 2020; Paton, et al., 2020; Renteria and Arellano, 2021). The second phase arises once governments have deal with the pandemic and try to learn from the lessons extracted and implement the necessary measures to mitigate the impact of the crisis (Boin and Hart, 2020).
In this article we focus on the first phase in which various governments such as the Norwegian, the Indian, or the Mexican, adopted similar measures recommended by the World Health Organization (WHO), such as isolation, restriction of movement, maintaining an adequate distance between people, among others (cfr. Jahagirdar et al., 2020; Christensen and Laegreid, 2020). In the Mexican case the first phase took place from February 27, when the first case appeared, until June 1, when the second response phase began; his implied to implement coordination efforts in a fragmented health system (Culebro, Méndez and Cruz, 2019) at different levels.
As noted, before we argue that a fragmented organizational / institutional design has an impact on crisis management, unlike other nations where the central government implemented extraordinary and unusual decisions to safeguard citizen well-being, managed to implement a kind of measures and regulations created to prevent the spread of the virus (Christensen and Laegreid, 2020). Besides, the use of symbols, such as solidarity, empathy, among others, as well as the perspective of collaboration between politicians, scientists, citizens, the media, and levels of government were important despite any controversies with local governments (cfr. Christensen and Laegreid, 2020).
Throughout this article, the concepts of crisis, crisis management and coordination are used on a regular basis to explain the response of local/subnational governments in Mexico. Regarding the first, it is generally associated with the concept of disaster, although they depart from different ideas, the disaster occurs when an event causes damage people and infrastructure due to natural causes such as earthquakes and floods, or by causes attributed to the individual such as terrorist attacks, economic losses, and technology failures (Boin, Hart and Kuipers, 2018). Meanwhile, the crisis refers mainly to an event, shared perception, or socio-linguistic construct about a latent threat in basic structures, norms, and fundamental values such as life or health; and therefore, it is necessary to act as soon as possible to reduce its impact (Backman and Rhinard, 2017; Boin, et al, 2005; Christensen et al, 2016; Matthews, 2012). Crisis management is an essential activity of the government to strengthen the resistance of the population, as well as the infrastructure networks (Baubion, 2012). Thus, management is seen as the sum of activities aimed at minimizing the impact, not only in the mentioned aspects, but also in public institutions (Boin, Kuipers and Overdijk, 2013), so that an appropriate management can be the difference between an incident or complete disaster (Boin, Hart and Kuipers, 2018).
In the first part, the concepts of crisis and coordination are reviewed, as well as interactions with crisis management and public sector as a model to study the Mexican case. Subsequently, the federal strategy is analyzed, so that in the following section the main characteristics of the policies and programs of the subnational governments are exposed, the case of the México City and the State of México. In the fourth section, the coordination instruments generated by federal and local strategies are discussed. Finally, in the conclusion section contributions are posed in terms crisis management for COVID-19 and organization theory, more specifically the way in which we employ two cases where subnational governments have deployed coordination instruments and by doing, so we advance our knowledge how coordination operates in a context of crisis within a fragmented system. In the next section we will develop the key concepts of the article, in particular coordination and its relationship with crisis management and public policies.
I. CRISIS AND COORDINATION
Coordination in crisis management has been an important issue, either with a different role in each of its stages, or to explain some types of crises, such as the transboundary crisis that crosses political and geographical borders. Transboundary crises demand international collaboration between levels of government and the employment of regulatory instruments, becomes a great challenge for the capacities of the State and government organizations. Moreover, cooperation and coordination are also relevant when it comes to the internal security of each country as in the case of terrorist attacks (Christensen et al., 2015) and floods (Jann et al., 2019). In a more interconnected world, the nature and characteristics of crises tend to produce different arrangements and instruments for coordination between sectors affected by disasters or emergencies (Blondin and Boin, 2020; Olsson, 2015).
The literature on coordination recognizes at least two main dimensions, the first one related to public policies and relevant to the solution of complex problems, even those called wicked problems (Peters, 2018). This dimension emphasizes the problems of integration of public programs for the implementation of public policies (Peters, 2018). From this approach, coordination is achieved mainly by hierarchy or through networks. The second dimension refers to organizational theory, which has deeply studied the various mechanisms of inter- and intra-organizational coordination either from the way of functioning and the context in which organizations operate (Mintzberg, 1993; Foss, 2020) or as a form of collaboration derived from the specialization of work in organizations (Culebro, 2000; Burton and Obel, 2018).
Fragmentation could become the other side of the coin when talking about coordination related to the coherence and integration of public policies and making decisions aimed to solve complex problems (Cejudo and Michell, 2017). For wicked problems for instance coordination and collaboration between levels of government becomes a precondition for its diagnosis and solution (Christensen et al., 2019). In the case of health systems such as Mexico, the problem of fragmentation is even more evident, not only because of the characteristics of the health system but also since the recent reforms that have taken place in Mexico in latest years. For instance, problems of fragmentation and weak coordination in the implementation of public programs related to nutrition in Mexico have been notorious (Delgado and Culebro, 2019); other situations of institutional design such as the tension between centralization and decentralization in the response to COVID-19 have also been important (Mattei and del Pino, 2021). Though, it does not happen in the same way in the case of interorganizational relationships (Marín-Idárraga and Campos, 2015).
Because of the administrative reforms, the importance of coordination, as a process or outcome for the public sector has been highlighted in the last decades, not only from the organization analysis (Mintzberg, 1993) but also for policy analysis and public sector performance (Bouckhaert et al., 2016). Furthermore, recent reforms associated with the Post-NPM approach have addressed the status of the coordination instruments to tackle with some fragmentation and atomization problems derived from the NPM reforms (Culebro, 2008) or those related to the Whole of Government Approach (Christensen and Laegreid, 2011) or Joined Up Government (Halligan, 2010). Sometimes through collaboration at the horizontal and vertical levels, or through the introduction of new ways of operating between agencies under the approach of performance measurement systems. In the context of such reforms, specialization of the public agencies appears to be one of the main causes of the absence of coordination.
As a result of these reforms, the specialization of public agencies has led to a debate about the necessary balances in the functioning and operation of the public sector, the first of these being related to the tension between the necessary autonomy of the agencies with purpose. unique and where appropriate with a regulatory function with the indispensable control; The second of the debates has brought the discussion around two forces, on the one hand centralizing efforts and on the other decentralization; In all these debates, coordination plays a fundamental role (Peters and Savolie, 1996, Christensen and Laegreid, 2006).
These potential tensions have come to affect the coordination processes between specific sectors such as food safety coordination. as a form of interorganizational coordination characterized by the establishment of exchange of information and rules in decision processes. A first form of coordination lies in the hierarchy with formal authority through planning instruments, while coordination through networks involves sharing information and is generally more flexible and horizontal. (Lie, 2011) Although, different forms of coordination can be established, in our case we use it as specific form of collaboration to align objectives and goals within public sector, aimed at strengthening greater coherence and reduce divergences between policies (Boukhaert and Peters, 2010),
During crisis management the significance of coordination acquires a different dimension and implications for governance (Christensen, 2016). The output of such interest lies on the fact that issues such as legitimacy and leadership have become essential to understand the policy responses for many governments, either to analyze the effects of health policies, or to understand the role of the authorities and the political context in the effectiveness of policies aimed at reducing the impact of the crisis. For instance, it has been noted that not only the lack of specialized resources, but also the absence of coordination instruments plays a key role in the emergencies such as those related with the current health crisis (Fannelly et al., 2020).
When it comes to crisis management, coordination instruments take on different roles depending on the type of crisis in question, be it in the case of disasters and responses in emergency situations. In these situations, some of the coordination mechanisms tend to be much more flexible even though in normal situations they may even be more formal and bureaucratic. Coordination, in a crisis context, refers to vertical and horizontal cooperation between various actors and organizations, to generate a coordinated behavior capable of effectively implementing the policies or decisions designed to face a critical event, despite the presence of behaviors and routine practices in organizations (cfr. Boin, Hart and Kuipers, 2018).
As a government action, crisis management plays an essential role in promoting the resilience of populations and critical infrastructure networks (Baubion, 2012). It can be defined as the sum of activities aimed at minimizing the impact of the crisis in terms of damage to the population, the infrastructure, or public institutions (Boin, Kuipers, and Overdijk, 2013). This type of management has a direct effect on citizens’ lives and social welfare, and when threats and vulnerabilities are not properly evaluated and addressed, a crisis will surely follow (Boin et al., 2005); moreover, it can save lives, protect infrastructure, and restore confidence in public institutions (Boin, Kuipers, and Overdijk, 2013). Crisis management effectiveness can be assessed based on ten executive tasks: early recognition; sense making; making critical decisions; orchestrating vertical and horizontal coordination; coupling and decoupling; meaning making; communication; rendering accountability; learning, and enhancing resilience (Boin, Kuipers, and Overdijk, 2013). Currently, the discussion focuses on a special type of crisis: the progressive crisis. Its effects are more devastating than those of other types of crises because, although they have been acknowledged for a certain length of time, no consequential actions have been taken, and they quickly transcend physical or administrative boundaries. Their potential harm is especially difficult to identify, they can be perceived as alien when first detected, and they cannot be effectively addressed using regular approaches, which challenges the governance model (Boin, 2020; Boin and Lodge, 2019).
Additionally, crisis management involves a diversity of actors from the private, public, or citizen sectors, with different interests, priorities, logics, and values (Boin, Kuipers and Overdijk, 2013). Many factors can affect the outcome of crisis management (Boin, Kuipers, and Overdijk, 2013), but coordination and cooperation issues are at the front line, especially when the crisis crosses borders of different kinds as the absence of goal achievement. Coordination involves horizontal and vertical joint actions involving multiple actors, organizations, and levels of government, as well as different policies that could be interacting for the first time. Although cooperation is identified as a major challenge for crisis management, it is also deemed as the essential solution to crises (Christensen et al., 2016; Boin, Kuipers and Overdijk, 2013). Coordination in the context of crisis management takes two forms; the first is structural-instrumental, and it refers to both the vertical relationship, i.e., hierarchical relations, and the horizontal relationship, which consists of alternative networks made by of same-level actors. In its cultural sense, coordination refers to the promotion of a cooperative culture (Christensen et al., 2007). Next, we will analyze the first phase of the policies and programs of the federal response to COVID-19, to later study the coordination instruments as reaction of the two states in Mexico.
II. COVID-19 CRISIS MANAGEMENT. THE FEDERAL STRATATEGY
A fundamental feature of Mexico’s health services is their high degree of fragmentation, expressed in the presence of various federal agencies responsible for serving different segments of the population. At the sub-national level, the fragmentation is greater. Since the 1997 decentralizing reform, the 32 entities have their own health agencies with their corresponding hospital systems where coverage is provided to both formal workers and those who are not in any federal social security institution (Culebro and Castro, 2017).
Organizationally, there are three levels of care –figure 1–. The first level, composed by Family Medicine Units, Health Centers and Family Clinics attends 80 % of basic health conditions. In the second are the general, regional, integral, community, pediatric, obstetric child hospitals, as well as the federal hospitals located in Mexico City as referents for the whole country. An expression of the Mexican political system is the great centralization of the country’s health infrastructure in Mexico City, linked to its status as the capital and head of the national urban system. Fragmentation is revealed in the co-existence of hospitals from two levels of government. At the federal level, there are hospital facilities of national public sector agencies in the City of México. At the subnational level of government, in Mexico City health services are provided through the Ministry of Health, in simultaneous competence with federal institutions –figure 2–; while in the State of Mexico it is done through the Ministry of Health of the State of Mexico and the Institute of Social Security of the State of Mexico (SSCDMX, 2017). At the regulatory level, the National Health System is composed of the agencies of the Federal public administration and subnational governments together with the individuals and companies of the social and private sectors that provide health services. At the subnational level, the state governments are also the health authorities. (DOF, 1984, Art. 5).
Figure 1. Agencies of the public sector at the federal and subnational level
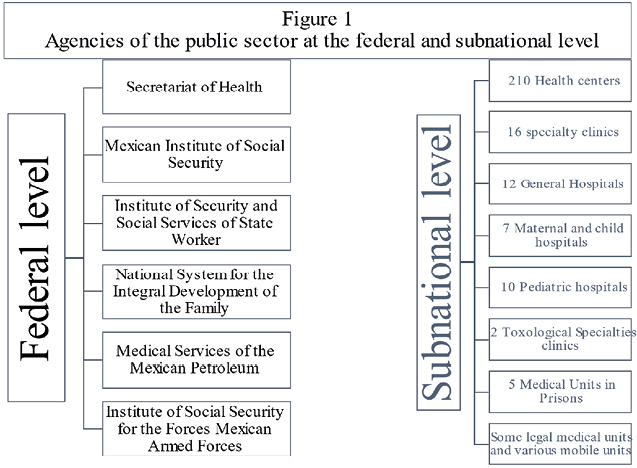
Source: Culebro, Mendez y Cruz (2019).
Figure 2. The health system of Mexico City
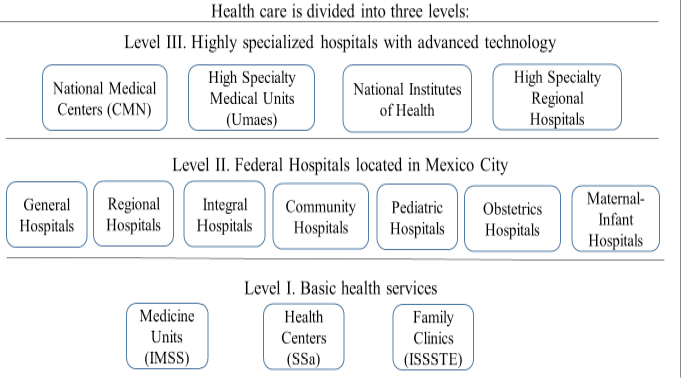
Source: Culebro, Mendez y Cruz (2019).
The Mexican health system is characterized by its fragmentation and inequality, basically it consists of three main dimensions: (1) a social insurance for workers in formal economy, this includes governmental employees, armed forces and employees for state owned companies, (2) public assistance services provided by INSABI and (3) a private sector; in addition, each federal entity has its own public health system.
Preparedness COVID-19 pandemic began in January 2020 with two main actions: increasing the installed hospital capacity and restricting activities to reduce the presence of people in the public space. From the epidemiological perspective, at least three phases have been developed in Mexico. The first infected patient was identified on February 28. On March 13, a three-stage management strategy began: generalized confinement, opening guided by an epidemiological traffic light, and vaccination. Hospital capacity was increased as Mexico moved into the second phase.
The first phase called the “National Campaign for Healthy Distance” was implemented officially from March 23 to May 30. It consisted in a set of preventive measures presented as mandatory, yet not coercive: individual rights were preserved and no state of exception or curfew affecting national residents or travelers in the country was decreed. Its purposes were to mitigate transmission, especially among the most vulnerable people, and to reduce the number of inpatients to guarantee access to health care in severe cases (DOF, March 24, 2020). The first infected patient was identified on February 28; on March 13, when the number of cases increased from 4 to 12, actions were intensified.
Restricted activities were a) Adults over 65 years of age and people at risk of developing a serious illness and/or dying as a consequence must avoid attending workplaces, public spaces, and other crowded venues...; b) School activities are suspended at all levels...; c) Temporarily suspend public, social, and private sector activities involving physical concentration, transit, or movement of people... (DOF, March 24, 2020).
These measures can be classified in three groups. The first group includes the suspension of activities in schools, public and private universities, and research centers for 10 weeks, from March 20 to May 30, to enable social distancing among 37.8 million students and teachers from all educational levels. Three subnational governments (Jalisco, Guanajuato, and Yucatán) suspended activities four days in advance, on March 17. Concerning the official calendar, the two weeks of Easter holidays were moved earlier and the complete suspension period was announced (SEP, 2020).
The second group refers to the temporary suspension of business activities (DOF, March 24, 2020). Approximately 6 million private companies employing more than 30 million employees stood down (INEGI, 2020). Shortly thereafter, measures became slightly more rigid, restricting the number of people inside supermarkets or allowing only pick-up meals in restaurants. The third group, which includes leisure activities, involved the cancellation of concerts, traditional religious festivities, mass celebrations in churches, and admission to movie theaters and soccer games, as well as access to sports stadiums, public parks, emblematic public squares, and pedestrian streets. The government’s invitation was summed up by the phrase “stay at home”.
Activities associated with the health sector, citizen security, the national guard, the army, and the navy were considered essential by the federal government. Security corporations continued carrying out their usual activities, appealing to persuasion to decrease the presence of people in public spaces and reduce the speed with which the virus spread, with the final goal of preventing the saturation of hospital facilities. In contrast, different countries such as Spain, Chile, the Dominican Republic, Venezuela, Colombia, El Salvador, Paraguay, Peru, and Puerto Rico resorted to different types of individual rights suspensions, states of exception, curfews, or complete lockdowns.
The capacity of the national health sector was increased by means of hospital reconversion (Secretaría de Salud, 2020b), purchase of specialized equipment, and coordination among federal health institutions and subnational organizations with the armed forces (SEDENA, SEMAR) and the hospital network operated by PEMEX, Mexico’s public oil company. An agreement with two national private hospital associations committed to pay for attention to patients not infected by COVID-19, which made it possible to increase the capacity of government hospitals to admit patients with COVID-19. Hospital capacity was also increased by two temporary hospitals installed in Mexico City, supported by business groups and advice from public universities. The federal government attempts to deal with the issue transparently by relying on groups of specialist physicians and researchers from public institutions, who created a statistical prediction model, and the COVID-19 MEXICO database was updated daily. Health authorities visited companies to ascertain the temporary suspension of activities.
As of May 30, a federal decree (DOF, May 14, 2020) established guidelines including a traffic light system for subnational government agencies, as health authorities, to take on the reopening process toward the “new normality”. The federal government committed to continue providing detailed information and projected scenarios. When this was announced, on May 20, urban mobility increased gradually in some cities as a result of the increase in individual economic activities and authorizations granted by subnational or municipal governments, despite that the National Campaign for Healthy Distance was not yet completed. While discussing it with subnational governments, as health authorities, if it was agreed that each government will calculate by color. State traffic lights have been agreed that may increase protection measures, regarding the federal traffic light.
These measures removed close to 80 million people from public space, equivalent to two thirds of the total national population during the first 3 months. This percentage was like that achieved by countries whose police restricted citizen mobility, in a country where 56.2 % of the population is involved in informal economy activities (INEGI, 2020). To facilitate health care, a policy by the government established the obligation to receive patients in any of the federal government hospital facilities, which broke the historical exclusion by entitlement in each of them. In what follows the response of the subnational strategy is presented aimed at analyzing the coordination instruments with the federal government.
III. THE RESPONSE OF THE SUBNATIONAL GOVERNMENT
From a more general level, the global health system comprises the constellation of actors (individuals and / or organizations) aimed at promoting, restoring, and maintaining health, as well as the connected laws that limit behavior, restrict activity from the community level, national or global, and that also includes governmental, intergovernmental, private for-profit and social organizations (Szlezak, et al., 2010). For the WHO, meanwhile, health systems are made up of various blocks among which are, (i) provision of services, (ii) health personnel, (iii) health information systems, (iv) access to medicines essentials, (v) financing and (vi) leadership / governance (WHO, 2010). At a global or national level, health systems are undergoing transformation and depend to a great extent on the historical trajectories of the countries, as well as on the administrative political context in which they are located. In this way, subnational health systems in Mexico are part of a set of institutions characterized not only by their fragmentation both horizontally and vertically, but also by their great inequality between regions and sectors (Bode and Culebro; 2018). At the subnational level, health systems replicate, on the one hand, the federal scheme, and on the other, they are capable to design their own organizational schemes. The health system of the subnational governments in Mexico is part of a much more complex health system that was undergoing transformation at the time of the crisis. In Mexico City, the Secretary of Health of Mexico City is responsible for planning, organizing, operating, controlling, and evaluating the Health System, as well as for organizing and executing programs and actions for health regulation and control. in matters of local health..., whose coordination oversees the Major of the Government of Mexico City, both the administrative units and the hospitals, clinics and health centers While the State of Mexico, is the Secretariat of Health del Estado de México is in charge of health in the State, although the provision of health services is the responsibility of a decentralized body, the Instituto de Health of the State of Mexico. In this way, the two health systems become different in terms of their organization, but similar in their relationship with the federal health system.
In Mexico City, the country’s capital, coordination mechanisms involving the citizenry were implemented so that a patient could dial 911 and be assigned a hospital bed in any medical unit. The Head of Government, in coordination with the Secretariat of Health, was responsible for directing actions to address the crisis in Mexico City (Sedesa). The capital’s health care system is in better shape than in other states, although coordination among its agencies is fraught with problems (Culebro et al., 2019). Municipal governments adopted secondary measures to support the strategy. In preparation for the return to activities a gradual plan toward the new normality was issued in Mexico City (Gobierno de la Ciudad de México, 2020).
At the beginning of the crisis, Mexico City’s Head of Government and State of Mexico’s Governor agreed share hospitals and work in coordination to facilitate the admission of patients to the nearest hospital or the one with availability during the first wave, regardless of the residence entity. For instance, in Mexico City, approximately 30 % of those hospitalized were residents of a municipality in the state of Mexico. These two subnational governments administer the metropolitan area in the Valley of Mexico, home to 20 million people and the place where the largest number of contagious cases was registered at the national level. An outcome of this coordination was the construction of two temporary hospitals.
In the State of Mexico, governmental decisions were focused on four aspects: closure of commercial venues, mandatory use of face masks, supervision of activities, and creation of regulations. Due to space restrictions, we will refer to the first two only. On March 22, the government began to close its modules and offices; however, citizens’ procedures were unaffected, since penalties were waived, and the validity of driver’s licenses was overridden for the rest of the month and until April 204.
This mandatory closure included different public spaces such as libraries, museums, and day-care centers for children and the elderly, among others, but also private businesses such as shopping centers, bars, nightclubs, and other non-priority establishments, that is, businesses whose products or services were not of immediate need (Jacinto, 2020). To ensure compliance with the measure, the government implemented special operations to temporarily close a number of public, private, and social sector agencies5, and imposed fines and penalties to companies that failed to comply with the mandate (Navarro, 2020). However, initially, these operations were limited to the control of access to supermarkets and street markets by restricting entry to one out-of-risk person per family wearing a face mask and using antibacterial gel. As an additional preventive measure, on April 8, the government encouraged people to wear face masks when they went outside6. When this measure was approved, on April 21, it was established as mandatory once the third phase of the epidemic was declared at the federal level. People would be required to use face masks when leaving their home and when using public transportation (Navarro, 2020), which would reduce its operating capacity by 50 % (GEM, 2020). Despite the coordination measures and actions, the State of Mexico governor was a secondary actor.
In this first stage of COVID-19 crisis management, vertical and horizontal coordination, as well as the behavior of the two subnational governments was relevant. Due to partisan affinity with the federal government in Mexico City, the ruler not only adopted the federal discourse and measures, but also promoted federal policies, although later she had some discrepancies with the federal approach. In the state of Mexico, an opposition party rules the State, and the governor assumed the federal discourse and strategy.
An interesting phase began on June 1, when the national decree ratifying the federal hierarchy established by the General Health Law was signed, establishing the National Campaign for Healthy Distance. From that moment on, based on federal-level information, the traffic light model prediction and logistic support, each of the 32 subnational governments, including the City of Mexico and the State of México determined the step at which their activities will resume in each municipality, using their powers as health authorities.
CONCLUSIONS
The development of coordination instruments in the health system in Mexico has become a story like a pendulum that goes from centralization to decentralization of functions within a design that has generated conflicts between the different levels of government, and above all in public health areas (Nigenda et al., 2015). On the one hand, the article complements studies on coordination in the first responses that countries have faced to reduce the impact of the crisis in multilevel governments (Mattei and Del Pino, 2021); and on the other, the importance of administrative capacity and leadership of the authority to balance the first decisions with the instruments of governance and legitimacy during a health crisis (Christensen and Laegreid, 2020).
Analysis was developed with the use of crisis management approach that highlighted the role of the government in the first phase of the response. Thus, by combining crisis management approach with perspectives on coordination the study shows the role of subnational governments in dealing with crisis. The study also reveals the potential of crisis management and organization theory approaches to study health policies (Bode and Culebro, 2018) and those related to pandemic crisis, in which vertical and horizontal coordination co-exist in different political systems, either in comparative studies or at subnational level (Liu et al., 2021).
In general terms, despite an eroded health system and their fragmentation, as of May 30, the authorities were aimed at reducing the impact of the crisis. Even though there was a great effort to generate coordination instruments as strategies for crisis management, coordination was still weak in a context of transformation of the health system in Mexico and austerity policies at the federal level. In this first stage, the centralism that has characterized the Mexican system allowed the federal government to operate a strategy that was adopted by subnational governments. It was a coordination through a vertical hierarchy that achieved compliance close to 85 %7. Even though coordination difficulties may arise in later stages.
The COVID-19 epidemic hit the country two months after its outbreak in other countries; therefore, it was possible to prepare in advance through different measures. Among other things, the collapse of the hospital network was prevented during this first stages, though later the percentage of available space in hospitals reduced dramatically. Once the reopening phase was announced there were 14,583 COVID-19 patient care beds available and 65 % care beds equipped with a ventilator; the official number of positive cases was 81,400 –active 16,315– and 9,044 people had died (Comunicado Técnico Diario, 2020). One form of coordination was through patient care independent of their affiliation through the necessary financial adjustments. This situation was repeated in the hospitals of 24 States, which in February 2020 agreed to sign an agreement for INSABI to be responsible for hiring new health personnel, medicines, assuming responsibility for the administration and provision of health services8. These actions allowed us to glimpse the possibilities of creating a Unified Health System of a public, universal and free (Laurell, 2020), opening the debate on the areas in decentralization processes (Falleti, 2010; Tulchin, 2012) its efficiency (Gallego, 2016) and political implications (Aalen and Muriaas, 2017; Simonet, 2016) and the processes of recentralization of functions under various forms (Riedl and Dickovick, 2014; Dickovick and Eaton, 2013).
The article contributes to the study of the first responses to face the COVID-19 crisis. In the field of literature on organization theory, the Mexican experience suggests that despite political and ideological considerations, organizations develop their own coordination mechanisms in the face of dynamic and complex contexts (Mintzberg, 1993; Foss, 2020); in some cases, as part of previous interactions as in the case of the metropolitan area of the Valley of Mexico, but also as a form of adaptation and learning from the environment (Levit and March, 1988). One way of observing this issue is to reflect about the nature of coordination to face a crisis, for example by including different coordination instruments depending on the stages of the crisis. Under the new institutionalism approach the article highlights the importance of the features of the political-administrative system in Mexico for the first responses of the federal government, if these responses influence subsequent policies (Bode and Culebro, 2018). Similar to the pragmatic approach in crisis management (Boin and Lodge, 2021b) the federal and the subnational governments in México did not impose severe measures that may affect severely mobility or the use of armed forces.
Crisis management and its strategic tasks, undertaken by organizations at different government levels, present differences, but also similarities. Among the similarities, the use of vertical coordination was observed. The relationships between the federal and subnational governments and between the latter and local governments suggest the presence of a generally accepted hierarchy. The dichotomy between control and autonomy in vertical levels seemed to play an important role, as long as, subnational governments were able to manage their own policies. Particularly, when it comes a weak coordination.
On the other hand, communications and sensemaking highlighted a remarkable difference: in this regard, the Federal government and the Mexico City governments played more significant roles compared to the State of Mexico government. Other differences and similarities are due to organizational and institutional aspects and crisis management approaches, but further analysis in this regard will be necessary as this human catastrophe continues unfolding.
The crisis management approach was found to be useful in understanding coordination mechanisms, especially in the context of a progressive crisis whose subsequent stages will have a deep impact on economic and social life besides the health-related matters. The cases presented point out that despite having a fragmented health system and a context where sub-national governments come from different political parties, including those opposed to the federal one, coordination can be generated by means of the creation of adequate meaning, driven daily by the federal government; the political will for cooperation due to the sharing of political borders in a megalopolis; and the passivity or inactivity of a political leadership.
The article shows on the one hand that coordination among different levels of government do not depend on political affinities but consist of a blend of weak and suitable articulation of policies of the subnational governments; an on the other the need to improve the instruments of collaboration between the various levels of government in the context of a healthcare system in transformation.
Most of the government’s responses sought to create vertical and horizontal coordination instruments, at least for the metropolitan area of Mexico City. Although the institutional design of the political administrative system influences the responses of governments at different levels, the dilemma is, on the one hand, to find strategies that reward adequate coordination in fragmented and highly unequal health systems, and on the other hand, to resolve the tensions that can occur transversally with other areas such as the economy and employment, among others. The article contributes to the study of multilevel governance in metropolitan areas (Schurgelies and Baines, 2016) by assessing coordination problems in health institutions, managed simultaneously with problems of transportation, employment, marginalization, among others.
REFERENCES
, & (2017). Power calculations and political decentralisation in African post-conflict states. International Political Science Review, 38(1), 56-69. https://doi.org/10.1177/0192512115615704
, & (2017). The European union’s capacities for managing crises. Journal of Contingencies and Crisis Management, 26(2), 261-271. https://doi.org/10.1111/1468-5973.12190
(2012). OECD Risk Management: Strategic Crisis Management [OECD Working Papers on Public Governance No. 23]. OECD. https://doi.org/10.1787/5k41rbd1lzr7-en
, & (2020). Cooperation in the face of transboundary crisis: A framework for analysis. Perspectives on Public Management and Governance, 3(3), 197-209. https://doi.org/10.1093/ppmgov/gvz031
, & (2018). Paradoxical Internationalization: Regulatory Reforms in the Mexican Health-Care System through the Lens of European Experience. Politics & Policy, 46(4), 678-710. https://doi.org/10.1111/polp.12268
(2020). Hiding in Plain Sight: Conceptualizing the Creeping Crisis. Risk, Hazards & Crisis in Public Policy, 11(2), 116-138. https://doi.org/10.1002/rhc3.12193
, , & (2018). The crisis approach. In H. Rodriguez, W. Donner, & J. E. Trainor (Eds.), Handbook of Disaster Research [Handbooks of Sociology and Social Research]. Springer International Publishing.
, , & (2013). Leadership in times of crisis: a framework for assessment. International Review of Public Administration. 18(1), 79-91. https://doi.org/10.1080/12294659.2013.10805241
, , & (2005). The Politics of Crisis Management. Cambridge University Press.
, & (2019). The twilight zone between crisis and risk management. Encompass. https://encompass-europe.com/comment/the-twilight-zone-between-crisis-and-risk-management-why-government-needs-to-pay-attention-to-creeping-crises#:~:text=These%20new%20challenges%20are%20emerging,between%20crisis%20and%20risk%20management.&text=These%20creeping%20crisis%20fall%20between,of%20crisis%20and%20risk%20management
& (2020). Beyond COVID-19: Five commentaries on expert knowledge, executive action, and accountability in governance and public administration [chapter: Shaping the long shadows of COVID-19: three challenges for Governments]. Canadian Public Administration, 63(3), 339-368.
, & (2021a). The Attractions and Limitations of Pragmatist Crisis Management: A Discussion in Light of COVID-19 Experiences. LSE Public Policy Review, 1(4), article 9. http://doi.org/10.31389/lseppr.22
, & (2021b). Responding to the COVID-19 crisis: a principled or pragmatist approach? Journal of European Public Policy, 28(8), 1131-1152, https://doi.org/10.1080/13501763.2021.1942155
, , & (2010). The Main Argument – Specialization without Coordination is Centrifugal. In: The Coordination of Public Sector Organizations [Public Sector Organizations book series]. Palgrave Macmillan. https://doi.org/10.1057/9780230275256_1
, , & (2016). Coordination of public sector organizations [Public Sector Organizations book series]. Palgrave Macmillan.
, & (2018). The science of organizational design: fit between structure and coordination. Journal of Organization Design, 7, article 5/2018. https://doi.org/10.1186/s41469-018-0029-2
, & (2017). Addressing fragmented government action: Coordination, coherence, and integration. Policy Sciences, 50(4), 745-767. https://doi.org/10.1007/s11077-017-9281-5
, , , & (2016). Comparing coordination structures for crisis management in six countries. Public Administration, 94(2), 316-332. https://doi.org/10.1111/padm.12186
, & (2019). Administrative coordination capacity; does the wickedness of policy areas matter? Policy and Society, 38(2), 237-254. https://doi.org/10.1080/14494035.2019.1584147
, & (2020). The coronavirus crisis-crisis communication, meaning-making, and reputation management. International Public Management Journal, 23(5), 713-729. https://doi.org/10.1080/10967494.2020.1812455
, & (2011). Post-NPM reforms: whole of government approaches as a new trend. In Groeneveld, S., & Van De Walle, S. (Eds.), New steering concepts in public management [Research in Public Policy Analysis and Management] (vol. 21, pp. 11-24). Emerald Group Publishing Limited. https://doi.org/10.1108/S0732-1317(2011)0000021006
, & (2020). Balancing governance capacity and legitimacy: how the Norwegian government handled the COVID-19 crisis as a high performer. Public Administration Review, 80(5), 774-779. https://doi.org/10.1111/puar.13241
, & (Eds.). (2006). Autonomy and regulation: Coping with agencies in the modern state. Edward Elgar Publishing.
, , & (2015). The challenges of coordination in national security management–the case of the terrorist attack in Norway. International Review of Administrative Sciences, 81(2), 352-372. https://doi.org/10.1177/0020852314564307
, , & (2016). Organizing for crisis management: Building governance capacity and legitimacy. Public Administration Review, 76(6), 887-897. https://doi.org/10.1111/puar.12558
, , , & (2007). Organization Theory and the Public Sector. Instrument, culture and myth. Routledge.
, , & (2019). Coordination and regulation in crisis management. Response of the health sector to disasters. The case of the 2017 earthquake in Mexico City. International Public Management Review, 19(2), 47-65. https://journals.sfu.ca/ipmr/index.php/ipmr/article/view/359
(2000). Cambio Estructural. In D. Arellano, E. Cabrero, & A. del Castillo (coords.), Reformando al Gobierno. Una visión del cambio en las organizaciones gubernamentales. Porrúa.
(2008). Atomización del Estado y nuevas formas de control: La introducción de los convenios de desempeño en organizaciones públicas. Gestión y política pública, 17(1), 35-70. http://www.gestionypoliticapublica.cide.edu/num_anteriores/Vol.XVII_No.I_1ersem/02_Jorge_Culebro.pdf
, & (2017). Reforma administrativa a los Sistemas de Seguridad Social. El caso del Estado de México (2017). Una propuesta para su estudio. In M. Lara, & J. de la Rosa (Eds.). Evaluación de Políticas Públicas (pp. 66-78). Ed. Juan Pablos. UAM-Lerma.
, & (2019). Política social y transferencia de políticas públicas. Coordinación y aprendizaje en la cruzada nacional contra el hambre en México. Revista de El Colegio de San Luis, 9(20), 215-239. https://doi.org/10.21696/rcsl92020191004
DIARIO OFICIAL DE LA FEDERACIÓN – DOF (2020, May 14). ACUERDO por el que se establece una estrategia para la reapertura de las actividades sociales, educativas y económicas, así como un sistema de semáforo por regiones para evaluar semanalmente el riesgo epidemiológico relacionado con la reapertura de actividades en cada entidad federativa, así como se establecen acciones extraordinarias. https://www.dof.gob.mx/nota_detalle.php?codigo=5593313&fecha=14/05/2020
DIARIO OFICIAL DE LA FEDERACIÓN – DOF (2020, March 24). Acuerdo por el que se establecen las medidas preventivas que se deberán implementar para la mitigación y control de los riesgos para la salud que implica la enfermedad por el virus SARS-CoV2 (COVID-19). https://www.dof.gob.mx/nota_detalle.php?codigo=5590339&fecha=24/03/2020
DIARIO OFICIAL DE LA FEDERACIÓN – DOF (1984, February 7). Ley General de Salud. http://dof.gob.mx/nota_detalle.php?codigo=4652777&fecha=07/02/1984
, & (2013). Latin America’s Resurgent Centre: National Government Strategies after Decentralisation. The Journal of Development Studies, 49 (11), 1453-1466, https://doi.org/10.1080/00220388.2013.797073
(2010). Decentralization and Subnational Politics in Latin America. Cambridge University Press.
, , , & (2020). Facing the Pandemic: The Italian Experience From Health Management Experts’ Perspective. The American Review of Public Administration, 50(6-7), 753-761. https://doi.org/10.1177/0275074020942428
(2020). The Impact of the Covid-19 Pandemic on Firms’ Organizational Designs. Journal of Management Studies, 58(1), 270-274. https://doi.org/10.1111/joms.12643
Gallego, R. (Dir.) (2016). Descentralización y desigualdad en el estado autonómico. Tirant lo Blanch.
GEM (2020). Servicios a medios. Comunicados. https://www.gem.gob.mx/medios/w2ls.aspx?tser=C
GOBIERNO CIUDAD DE MÉXICO (2020). Plan gradual hacia la nueva normalidad en la Ciudad de México. https://covid19.cdmx.gob.mx/storage/app/media/plan%20gradual%20hacia%20la%20nueva%20normalidad%20en%20la%20ciudad%20de%20mexico/plangradualhacialanuevanormalidadenlaciudaddemexico20.pdf
(2010). Post-NPM Responses to Disaggregation Through Coordinating Horizontally and Integrating Governance. In P. Lægreid, & K. Verhoest (Eds.), Governance of Public Sector Organizations. [serie Governance and Public Management] (pp. 235-254). Palgrave Macmillan. https://doi.org/10.1057/9780230290600_12
INSTITUTO NACIONAL DE ESTADÍSTICA Y GEOGRAFÍA (2020). Censos Económicos 2019. Resultados Oportunos. https://www.inegi.org.mx/contenidos/programas/ce/2019/doc/pro_ce2019.pdf
(2020). Edomex cierra bares, centros comerciales y cines por coronavirus. El Universal. https://www.eluniversal.com.mx/metropoli/edomex/coronavirus-edomex-cierra-bares-centros-comerciales-y-cines-por-covid-19
, , , & (2020). Response to the COVID-19 pandemic in India: Case studies on leadership in crisis situations. International Journal of Health & Allied Sciences, 9(5), 81-84. https://www.ijhas.in/article.asp?issn=2278-344X;year=2020;volume=9;issue=5;spage=81;epage=84;aulast=Jahagirdar
, , , & (2019). The flood crisis in Germany 2013. In P. Lægreid, & L. H. Rykkja (Eds.), Societal Security and Crisis Management (pp. 75-93). Palgrave Macmillan, Cham. https://doi.org/10.1007/978-3-319-92303-1_4
, , , & (2020). The nature of cities and the Covid-19 pandemic. Current Opinion in Environmental Sustainability, 46, 27-31. https://doi.org/10.1016/j.cosust.2020.08.008
(2020). Las dimensiones de la pandemia de COVID-19. El trimestre económico, 87(348), 963-984. https://doi.org/10.20430/ete.v87i348.1153
, & (1988). Organizational learning. Annual review of sociology, 14, 319-338. https://www.annualreviews.org/doi/10.1146/annurev.so.14.080188.001535
(2011). Coordination processes and outcomes in the public service: The challenge of inter-organizational food safety coordination in Norway. Public Administration, 89(2): 401-417. https://doi.org/10.1111/j.1467-9299.2010.01845.x
(2020, September, 10). ¿Hacia un Sistema Único de Salud? La Jornada. https://www.jornada.com.mx/2020/09/10/opinion/a03a1cie
, , , & (2021). Multi-Level governance, policy coordination and subnational responses to COVID-19: Comparing China and the US. Journal of Comparative Policy Analysis: Research and Practice, 23(2), 204-218. https://doi.org/10.1080/13876988.2021.1873703
, & (2015). Estructura organizacional y relaciones inter-organizacionales: análisis en Instituciones Prestadoras de Servicios de Salud públicas de Colombia. Estudios Gerenciales, 31(134), 88-99. https://doi.org/10.1016/j.estger.2014.08.004
, & del (2021). Coordination and health policy responses to the first wave of COVID-19 in Italy and Spain. Journal of Comparative Policy Analysis: Research and Practice, 23(2), 274-281. https://doi.org/10.1080/13876988.2021.1878886
(2012). Governance, Governing and the Capacity of Executives in Times of Crisis. In M. Lodge, & K. Wegrich (Eds.). Executive Politics in Times of Crisis. The Executive Politics and Governance series (pp. 217-238). Palgrave Macmillan.
(1993). Structure in fives: Designing effective organizations. Prentice-Hall, Inc.
, & (2020). Australian Quarantine Policy: From centralization to coordination with mid-Pandemic COVID-19 shifts. Public Administration Review, 80(4), 671-682. https://doi.org/10.1111/puar.13224
(2020, April 21). Por fase 3 de covid-19, Edomex pide sólo salir a comprar alimentos y medicinas. El Sol de México. https://www.elsoldemexico.com.mx/metropoli/valle-de-mexico/por-fase-3-de-covid-19-edomex-pide-solo-salir-a-comprar-alimentos-y-medicina-5133034.html
, , , & (2016). Understanding the dynamics of the Seguro Popular de Salud policy implementation in Mexico from a complex adaptive systems perspective. Implementation science, 11:68. https://doi.org/10.1186/s13012-016-0439-x
(2015). Transboundary crisis networks: The challenge of coordination in the face of global threats. Risk Management, 17(2), 91-108. https://doi.org/10.1057/rm.2015.9
, , , & (2020, May 25). Bolsonaro llama al coronavirus una “pequeña gripe”. Dentro de los hospitales de Brasil, los médicos conocen la horrible realidad. CNN en español. https://cnnespanol.cnn.com/2020/05/25/bolsonaro-llama-al-coronavirus-una-pequena-gripe-dentro-de-los-hospitales-de-brasil-los-medicos-conocen-la-horrible-realidad/
, , & (2021). Support for the measures in fighting the COVID-19 pandemic: The role of political ideology. Psihologija, 54(2), 207-222. https://doi.org/10.2298/PSI201027039P
(2018). The challenge of policy coordination. Policy Design and Practice, 1(1), 1-11. https://doi.org/10.1080/25741292.2018.1437946
, & (1996). Managing incoherence: The coordination and empowerment conundrum. Public Administration Review, 56(3), 281-290. https://doi.org/10.2307/976452
(1999). The distinctiveness of case-oriented research. Health services research, 34(5 Pt 2), 1137-1151. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1089057/
(2020, March, 21). Cdmx, Edomex y el gobierno federal crean mando metropolitano contra la propagación del covid-19. Animal Político. https://www.animalpolitico.com/2020/03/cdmx-edomex-mando-metropolitano-covid-19//
, & (2021). How does a populist government interpret and face a health crisis? Evidence from the Mexican populist response to COVID-19. Revista de Administração Pública, 55(1), 180-196. https://doi.org/10.1590/0034-761220200524
, , , , & (2020). City size and the spreading of COVID-19 in Brazil. PloS one, 15(9), article e0239699. https://doi.org/10.1371/journal.pone.0239699
& (2014). Party Systems and Decentralization in Africa. Studies in Comparative Internacional Development, 49(3), 321-342. https://doi.org/10.1007/s12116-013-9144-9
, & (2020, September 10). Trump sabía que el coronavirus era “mortal” y peor que la gripe, y engañó intencionalmente a los estadounidenses, según el nuevo libro de Bob Wordward. Washingtonpost. https://www.washingtonpost.com/es/politics/2020/09/10/trump-sabia-que-el-coronavirus-era-mortal-y-peor-que-la-gripe-y-engao-intencionalmente-los-estadounidenses-segun-nuevo-libro-de-bob-woodward/
SECRETARIA DE SALUD (2020a). Comunicado Técnico diario, 2020. Gobierno de México. https://www.gob.mx/salud/es/archivo/prensa
SECRETARÍA DE SALUD (2020b). Lineamiento de Reconversión Hospitalaria. Gobierno de México. Recuperado de: https://coronavirus.gob.mx/wp-content/uploads/2020/04/Documentos-Lineamientos-Reconversion-Hospitalaria.pdf
(2016). Recentralization and vertical alignment in the French healthcare system. Journal of Public Affairs. 17(4), article e1640. https://doi.org/10.1002/pa.1640
, & (2016). Improving metropolitan governance: A case study of the Greater São Paulo. Revista Eletrônica Gestão e Serviços, 7(1), 1561-1575. https://www.metodista.br/revistas/revistas-ims/index.php/REGS/article/view/6569
(1995). The art of case study research. Sage.
, , , , , , & (2010). The global health system: actors, norms, and expectations in transition. PLoS Medicine, 7(1), article e1000183. https://doi.org/10.1371/journal.pmed.1000183
(2012). Decentralization and its discontents. Latin American Research Review, 47(2), 191-199. https://www.jstor.org/stable/23321739
(2014). Research methods in public administration and public management: An introduction. Routledge.
WORLD HEALTH ORGANIZATION (2010). Monitoring the building blocks of health systems: a handbook of indicators and their measurement strategies. https://www.who.int/healthinfo/systems/WHO_MBHSS_2010_full_web.pdf
(1994). Discovering the future of the case study. Method in evaluation research. Evaluation practice, 15(3), 283-290. https://doi.org/10.1016/0886-1633(94)90023-X
1 The research was founded by the National Council of Science and Technology (CONACYT). Project #311798.
2 We want to thank the anonymous reviewers and the journal editor for their suggestions and comments on the first version of this article.
3 Since Mexico is a federal Republic. Here we use the term subnational governments to refer to the 32 States and Local government is used in reference to municipalities.